Do Babies Aspirate at Some Feeds and Not Others
Top of page
Key Points
- Normal development of feeding and swallowing is an important basis for understanding feeding and swallowing disorders in infants and children.
- Critical and sensitive periods are important considerations in developmental expectations for expanding textures in young children.
- Pertinent questions to determine if further investigation of feeding and swallowing is needed:
- If meal times takes more than 30 minutes on average.
- Are meal times stressful?
- Does the child show signs of respiratory stress?
- Has the child not gained weight in the past 2 to 3 months?
- Most children with complex feeding and swallowing problems are best served by an interdisciplinary team.
- Videofluoroscopic swallow study (VFSS) or flexible endoscopic examination of swallowing (FEES) are needed to define pharyngeal physiology with risks for aspiration or other pulmonary problems
- Intervention strategies must not jeopardize nutrition and hydration, nor should they be stressful to infants and children.
- Outcomes of therapy depend on multiple interrelating systems, including neurologic status, airway protection, and integrity of gastrointestinal (GI) tract.
Top of page
Introduction
Adequate respiration and nutrition are essential throughout a lifetime. Breathing usually does not require active effort by infants except for those with complicating factors, for example, bronchopulmonary dysplasia (BPD) leading to chronic lung disease (CLD), upper airway obstruction as in Pierre Robin sequence (PRS), other craniofacial anomalies, and severe laryngotracheobronchomalacia. Eating, on the other hand, requires active effort by infants who must have exquisite timing and coordination for sucking, swallowing, and breathing at the breast or bottle. Adequate growth, defined by weight gain in early infancy and for the first few years of life, is the primary measure of successful feeding. Feeding, swallowing, and respiration are activities that occur in the upper aerodigestive tract and are orchestrated by specific areas in the brain and cranial nerves. Successful oral feeding requires that children have functional oral sensorimotor and swallowing skills, overall adequate health (including pulmonary and gastrointestinal function), central nervous system integration, and musculoskeletal tone. A breakdown in coordination of swallowing and breathing can result in aspiration, which, over time, can progress to bronchiectasis. Aspiration may present with coughing and choking, usually during feeding, and is indicative of compromised airway protective reflexes. If laryngotracheal sensation is also affected, aspiration may be silent without any overt manifestations.
Successful emergence of communication skills relates to successful feeding and swallowing. Normal feeding patterns reflect the early developmental pathways that are the basis for later communication skills. The interrelationships between feeding (in all living beings) and complex verbal communication (unique to humans) are multifactorial and in need of continued research. The study of comparative anatomy and its implications for human communication are well described.1
Professionals who examine and treat infants and children who have feeding and swallowing problems must have a thorough understanding of embryologic and developmental anatomy of the upper aerodigestive tract and the physiology of deglutition. Research in the past 30 years has added to the understanding of the orderly development of feeding and swallowing in utero through infancy.
Top of page
Incidence and Prevalence of Feeding and Swallowing Disorders in Pediatrics
Feeding and swallowing disorders are relatively common in early infancy and in some instances may be markers for significant health implications that do not become obvious until later. As many as 35% of infants exhibit food selectivity and refusal, as revealed by parent interviews in general population surveys. Feeding problems are relatively common in various infant populations, including, but not limited to, preterm "at-risk" infants, infants with congenital heart disease following open-heart surgery, infants diagnosed with nonorganic failure to thrive, and children with cerebral palsy (CP). Prevalence rates of dysphagia range from 57% to 92% varying by type of CP.2 Children with CP and dysphagia are found to have a higher incidence of undernutrition, growth failure, and poor health than those children without swallowing problems. Children with more severe forms of CP and dysphagia have higher mortality rates than other groups.
This review provides an overview of (1) the development of feeding and swallowing skills, including critical/sensitive periods with implications for behavioral and sensory based feeding problems; (2) taste and smell, and their impact on oral feeding; (3) clinical assessment; (4) instrumental examination of pediatric swallowing disorders; and (5) management of pediatric feeding and swallowing disorders.
Top of page
Development of Feeding and Swallowing Skills
Prenatal Swallowing and Sucking
In utero studies of fetuses have documented the early development of swallowing and oral-motor function3 (Table 1). In utero swallowing is important for the regulation of amniotic fluid volume and composition, recirculation of solutes from the fetal environment, and the maturation of the fetal gastrointestinal tract.4 The pharyngeal swallow, one of the first motor responses in the pharynx, has been observed between 10 and 12 weeks' gestation.5 Recent studies have demonstrated swallowing in most fetuses by 15 weeks' gestation and consistent swallowing by 22 to 24 weeks' gestation.3
True suckling begins around the 18th to 24th week and is characterized by a distinct backward and forward movement of the tongue. The frequency of suckling motions can be altered by taste. Taste buds are evident at 7 weeks' gestation. By 12 weeks' gestation, distinctively mature receptors are noted. Self oral-facial stimulation usually precedes suckling and swallowing. Tongue cupping is seen by 28 weeks' gestation.
This backward and forward movement of the tongue in suckling is all that can be expected because the tongue fills the oral cavity at this stage of development. Backward movement appears more pronounced than forward movement. Tongue protrusion does not extend beyond the border of the lips. Serial ultrasound images have shown that suckling motions increase in frequency in the later months of fetal life.3 By 34 weeks' gestation, a healthy preterm infant likely suckles and swallows well enough to sustain nutrition strictly through oral feedings. Some healthy preterm infants may be ready to begin oral feeding by 32 to 33 weeks' gestation.
It has been estimated that the near-term human fetus swallows 500 to 1000 mL/day of amniotic fluid.4 Earlier reports had indicated that the fetus swallows about 450 to 500 mL of amniotic fluid per day (of the total 850 mL) and excretes about the same amount in urine.6 Decreased rates of fetal suckling are associated with digestive tract obstruction or neurologic damage. Intrauterine growth retardation may be a manifestation of neurologic damage. Lack of regular swallowing by the fetus should lead one to suspect problems that may be related primarily to the preterm infant or primarily to the mother. Maternal polyhydramnios characterized by excessive amniotic fluid in the uterus may result from multiple fetal and maternal etiologies. Severe polyhydramnios is more strongly associated with congenital malformations than mild or moderate polyhydramnios.7
Infant Feeding and Swallowing
Oral feeding that requires suckling, swallowing, and breathing coordination is the most complex sensorimotor process the newborn infant undertakes. Premature infant patterns differ from those of full-term infants. Five primary developmental stages of sucking characterized the maturational process (Table 2).8 Sucking patterns in infants born at less than 30 weeks' gestation were monitored from the time they were introduced to oral feeding until they reached full oral feeding. The five-stage scale demonstrates the relationship between the development of sucking and oral feeding performance in preterm infants. A high interobserver reliability was observed on 50 bottle-feeding assessments. The authors suggest that there is no significant in utero maturation of sucking occurring between 26 and 29 weeks' gestation, or they had insufficient statistical power to detect a difference over this developmental period. A significant correlation between the level of maturity of an infant's sucking and gestational age was found. Feeding performance correlated with progression of oral feeding. These authors suggest that developmental scales can be used clinically for the identification and characterization of the oral sensorimotor skills of preterm infants at any point in their development as they progress in their individual oral feeding schedule. Objective and quantitative evaluations of infants' nonnutritive and nutritive sucking would be helpful in evaluating strength and coordination. One proposal includes a finger pressure device to allow for quantification of specific measures of nonnutritive sucking in combination with a nipple/bottle system developed for monitoring nutritive sucking.9 However, there is no standardized quantifiable procedure available currently.
Term infants typically show food-seeking behavior through rooting for a breast or other nipple for bottle feeding. Preterm infants gradually achieve skills for rooting, suckling, and swallowing for functional oral feeding as they advance toward term. Important early developmental milestones and feeding skills from birth to 36 months are shown in Table 3. Children older than 36 months typically are eating regular table food and drinking from an open cup. They continue to refine their skills, but they do not attain new skills. Thus, this review focuses on feeding and swallowing in infants and young children.
The development of independent, socially acceptable feeding processes begins at birth and progresses throughout the first few years of childhood. Oral sensorimotor skills improve within general neurodevelopment, acquisition of muscle control that includes posture and tone, cognition and language, and psychosocial skills (Table 3).10
Feeding and swallowing skill development parallels psychosocial milestones of homeostasis, attachment, and separation/individuation (Table 4).11 Infants during the first 2 to 3 months of life strive toward homeostasis with the environment. Goals include sleep regulation, regular feeding schedules, and awake states that are developmentally advantageous in the development of emotional attachment to primary caregivers. Successful pleasurable feeding experiences foster efficient nipple control, reaching, smiling, and social play. Thus, feeding gradually becomes a social event. Caregivers should not interpret pauses between sucking bursts as a need for burping or early satiety. Once caregivers interrupt feeding, some infants do not resume sucking readily. Caregivers then may perceive that an infant is full or too tired to continue, so they stop the feeding. If this pattern becomes habitual, the infant is likely to gain weight slowly or not at all, which results in undernutrition or failure to thrive. If the interactions between infant and caregiver fail to develop appropriately, the infant may indicate lack of pleasure, loss of appetite, and, in severe forms, vomiting and rumination. Significant feeding problems can evolve out of a mismatch between infants' cues and caregivers' interpretations of the cues.
Transition Feeding
Infants show readiness for the transitional feeding period that usually begins around 4 to 6 months in typically developing infants, which also is the period of attachment for psychosocial milestones (Table 4).11 Transition feeding describes the readiness for and initiation of spoon feeding, usually with thin cereal mixed into breast milk or formula for most infants. Infant developmental skills that indicate readiness for spoon feeding include, but are not limited to, upright sitting with minimal support, midline head position maintained for several minutes without support, hand to mouth motor skills, dissociation of lip and tongue motions, and anatomic changes resulting in more space for the tongue within the oral cavity that allow for vertical motion of the tongue in addition to the previously restricted movements of "in and out" suckling. Over the next several months, infants gain oral sensorimotor skills for accepting thicker and lumpier food by spoon. Then, they move into a period of greater independence noted by finger feeding of easily dissolvable solid food. They gradually become more precise in picking up small pieces of food (or other objects), as they attain a pincer grasp with thumb and forefinger, which is expected by 10 to 12 months.
Critical and Sensitive Periods with Implications for Behavioral and Sensory-Based Feeding Problems
The concept of critical and sensitive time periods in overall human development is well documented in some areas of development and in animal research. Lorenz12 interpreted findings from animal embryologic studies to imply that there is a period during early development when the organism is primed to receive and perhaps permanently encode important environmental information. These interpretations do not mean that later learning cannot occur or that it is not important, but they do emphasize the possible significance of these early experiences.
Critical and sensitive periods are believed to exist in the development of normal feeding behavior. Descriptions of these critical periods typically focus on the introduction of chewable textures (Table 3). Children develop oral side preferences for chewing that relate to hand preferences in many instances. Chewing skills vary with textures. Children develop mature chewing skills for solid foods earlier than for viscous and pureed foods. However, it is common for children who have not mastered the timing and coordination for swallowing purees and other smooth food to be kept on those textures because caregivers may believe that these children are not ready for introduction of chewable food, which is not necessarily true. Children need to be introduced to solid foods at the most appropriate times. Children may reject solids upon initial presentation if they are introduced after the critical periods. The longer the delay in the introduction of solids, the more difficult it is for many children to accept chewable food. Withholding solids at a time when a child should be able to chew (6 to 7 months developmental level) can result in food refusal and even vomiting,13 which in turn may have a significant negative effect on nutrition and hydration status.
Studies in mice reveal that those fed a soft-feed (powdered) diet after weaning reduced synaptic formation in the cerebral cortex and impaired the ability of spatial learning (radial maze) in adulthood when compared with mice fed a hard-feed (pelleted) diet.14 Similar deficits may result from lack of experience and exposure to age-appropriate foods in humans, providing a conceptual framework to explain clinical observations of the challenges encountered in the learning of oral sensorimotor and other skills in children not fed during critical/sensitive periods for oral skill development. Perhaps when children have not been introduced to solid foods within the critical sensitive periods, broad aspects of development may be affected negatively. One may assume that these children missed not only this critical period for chewing, but also the underlying skills, which include trunk stability, head control, mobility of limbs, and mouthing experiences involving hands, fingers, and toys. Physiologic processes that are underpinnings for oral sensorimotor and swallowing skills, such as respiratory control, also have critical periods that can impact the feeding process.
Psychosocial development, personality, and environment are additional factors that must be considered for children with feeding issues. Some children may respond in aversive ways when presented with certain textures, tastes, or temperatures of food and liquid. These same children may be hypersensitive to tight clothes or tags on their clothes. They may not like to wear shoes. They may get upset when their hands get dirty, so they refuse to do finger painting and will not put their fingers into pudding or other pureed food.
Critical and sensitive periods may apply to the mother, with effects related to the potential for efficient feeding and global development of an infant.15 Maternal early contact with both preterm and term infants has been found to have a positive effect on the mother's attachment behavior and ultimately enhanced development of the infant.
Effects When Oral Feeding Is Not Possible in the Newborn Period
When infants with major physical and physiologic problems are prevented from initiating oral feeding in the same time frames as their more typically developing peers, many demonstrate prolonged delays and significant difficulty with oral feeding. In addition, significant variations are found in the form and function of the ingestive systems of age-matched healthy infants and at-risk infants. Ultrasounds revealed that fetal swallowing occurred most commonly in the presence of oral-facial stimulation. Hands were touching face and mouth. In some instances, fingers or thumbs were seen in the mouth. Perhaps some infants miss critical periods while still in the womb. Miller and colleagues3 postulate that prenatal development indices of emerging aerodigestive skills may guide postnatal decisions for feeding readiness and, ultimately, advance the care of medically fragile neonates. Clinicians must have knowledge regarding normal development in order to appreciate and understand the implications of differences in infants and young children with feeding and swallowing problems, which are likely to be just one or two pieces of a much larger and more complex puzzle. All aspects must be delineated in order to plan management strategies that will permit adequate nutrition without pulmonary issues and without stress to the child as well as to the caregiver.
Top of page
Taste and Smell in Oral Feeding of Infants and Young Children
Understanding an infant's awareness of taste and smell, along with responses to textures and temperature, is fundamental for clinicians of any discipline to determine the potential for acceptance of new foods. Physicians, dietitians, nurses, and therapists who guide parents when children are failing to thrive, or have limited range of foods in the diet, must examine the broad parameters that can impact on a child's feeding status. These experiences occur much earlier than many professionals would expect. Initial experiences with flavors occur prior to birth, because the flavor of amniotic fluid changes as a function of the dietary choices of the mother. Flavors from the mother's diet during pregnancy are transmitted to amniotic fluid, which are not only perceived by the fetus, but enhance the acceptance and enjoyment of that flavor in a food during weaning from the breast. The ability to detect additional tastes and flavors develops after birth. Thus, it is clear the early sensory experiences have an impact on the acceptance of flavors and foods during infancy and childhood.16
It has long been shown that human infants are born with a preference for sweet. Their sensory apparatus can detect sweet tastes. Tatzer and colleagues17 found that preterm infants fed exclusively via gastric tubes exhibited more nonnutritive sucking in response to minute amounts of glucose than to water solutions presented intraorally. Infants produced more frequent and stronger sucking responses when offered a sucrose-sweetened nipple compared with a latex nipple.18
Exposure to flavors in breast milk may serve to heighten preferences for these flavors and facilitate the weaning process. Some breast-fed infants are more willing to accept a novel vegetable upon first presentation than are formula-fed infants.19 Children who have been breast-fed for at least 6 months are also less likely to become picky eaters.20
The ability to detect and prefer a salt taste does not appear until infants are about 4 months of age. Animal model studies demonstrate that this developmental change may reflect postnatal maturation of central and peripheral mechanisms underlying salt taste perception.21 The preference that emerges at this age appears to be largely unlearned.
An example of the importance of early exposure to flavors is found in the acceptance of protein hydrolysate formulas by 7-month-old infants who had readily accepted this kind of formula when compared to their regular milk- or soy-based formula in the first couple months of life. These formulas are known by a variety of names depending on the company that produces and distributes them in the United States and in other countries throughout the world. A sensitive period in early infancy is suggested as at least one important factor, as shown by the finding that those infants 7 months and older avidly accept these formulas if they have experienced them during the first months of life. However, in marked contrast, 7- to 8-month-old infants who had no previous experience with hydrolysate formulas strongly rejected them and displayed extreme and immediate facial grimaces, similar to those observed in newborns in response to bitter and sour tastes.22
Professionals who make decisions regarding feeding of infants and young children have to consider multiple variables. Differences in flavor acceptance that occur from breast-fed to bottle-fed infants and that likely change over time reflect complex interactions of sensory and motor factors.
Top of page
Clinical Assessment of Pediatric Swallowing and Feeding Disorders
Screening Questions for Primary Care Physicians
There are four key questions that physicians and nurses in primary care can ask parents when an infant or young child presents at the office or clinic with parental concerns related to feeding. The answers help determine if a comprehensive clinical feeding and swallowing assessment is needed, even though the answers do not necessarily define the problem:
- How long do mealtimes typically take? If more than about 30 minutes on any regular basis, there is a problem. Prolonged feeding times are major red flags pointing to the need for further investigation.
- Are mealtimes stressful? Regardless of descriptions of factors that underlie the stress, further investigation is needed. It is very common for parents to state that they "just dread mealtimes."
- Does the child show any signs of respiratory stress? Signs may include rapid breathing, gurgly voice quality, nasal congestion that increases as the meal progresses, and panting by an infant with nipple feeding. Recent upper respiratory illness may be a sign of aspiration with oral feeds, although there may be other causes.
- Has the child not gained weight in the past 2 to 3 months? Steady appropriate weight gain is particularly important in the first 2 years of life for brain development as well as overall growth. A lack of weight gain in a young child is like a weight loss in an older child or adult.
Principles of Clinical Feeding Evaluation
The clinical evaluation of an infant or child with complex issues related to feeding and swallowing includes a thorough history, physical examination, and feeding observation. Instrumental assessments of swallowing may be needed following the clinical evaluation when concerns are noted regarding pharyngeal phase physiology and risks for aspiration with oral feeding. Most children are best served in the context of an interdisciplinary team. Unfortunately, such teams are available only in a limited number of medical centers in the United States and in other countries throughout the world. Information is provided that should be useful for physicians, dietitians/nutritionists, and other professionals who do not have an interdisciplinary team available. All professionals who work with these infants and children are urged to collaborate with appropriate colleagues, and to develop an interdisciplinary team to whatever extent is possible. Particular attention is paid to factors that are likely to interfere with adequate nutrition and hydration, because the most fundamental goals for all children relate to optimal status of nutrition and hydration.
Categories of Causes of Swallowing and Feeding Disorders
A careful reading of the medical, developmental, and feeding history is the first step that is critical to decision making. Swallowing and feeding disorders in infants and children are complex and can have multiple causes in various categories of disorders including, but are not limited to:
- Disorders that affect hunger/appetite, food-seeking behavior, and ingestion
- Anatomic abnormalities of the oropharynx
- Anatomic/congenital abnormalities of the larynx and trachea
- Anatomic abnormalities of the esophagus
- Disorders affecting suck-swallow-breathing coordination
- Disorders affecting neuromuscular coordination of swallowing
- Disorders affecting esophageal peristalsis
- Mucosal infections and inflammatory disorders causing dysphagia
- Other miscellaneous disorders associated with feeding and swallowing difficulties, for example, xerostomia, hypothyroidism, trisomy 18 and 21, Prader-Willi syndrome, allergies, lipid and lipoprotein metabolism disorders, and a variety of craniofacial syndromes.
Link and Rudolph23 have a detailed list of specific causes within each of the above categories.
Caregiver Perceptions of Feeding Problems
Each person involved with feeding and caring for a child is likely to have perceptions of the feeding status and problems that differ from other caregivers and professionals. Information is needed from more than one caregiver or professional involved with the child. Questions are formulated to delineate the feeding status as clearly as possible. The following questions go beyond the screening questions suggested earlier:
How long does it take to feed the child?
Prolonged meal/feeding times that are more than 30 to 40 minutes on a regular basis in most cultures is one of the major markers of some kind of feeding problem for infants and children of any age, whether infants are strictly nipple feeding or children are on a broader range of food and liquid. Prolonged meal times in isolation would not define the nature of the problem. Prolonged feeding times may relate to oral sensorimotor deficits, airway issues and risks for aspiration, and parent-child interaction or behavioral based problems.
Is the child independent for feeding or dependent on others to a greater degree than would be expected for age and overall developmental status?
Independent feeders usually, but not always, have better coordination for functional swallow production than those with neurologic etiologies that make it difficult to hold the head upright or to produce swallows without delay. Children with quadriplegic cerebral palsy who are dependent feeders may demonstrate reduced oxygen saturation during feeding.24 They are more likely to be silent aspirators than children with overall better neuromuscular strength and coordination.25
Is the child a total oral feeder?
If the answer is yes, is the nutrition status adequate? If the child is not a total oral feeder, are nutrition needs met by a combination of oral and tube feedings? Many caregivers perceive total oral feeding as a marker of success for the child as well as for parenting. However, if the child is at risk for undernutrition, tube feeding allows for nutrition and hydration needs to be met without placing undue risk on the respiratory system and/or the energy levels required for feeding orally, as well as parent-child interaction stress.
Do differences in food textures, temperatures, or tastes change the child's response at mealtime?
Aspiration and pharyngeal deficits can be texture-specific in some children. Children with anatomic abnormalities, such as esophageal webs, strictures, vascular rings, or enlarged tonsils and adenoids, may have difficulty progressing to solid foods. Children with incoordination of the oral and pharyngeal phases of swallowing or with a delay in initiating a pharyngeal swallow are at greater risk for aspiration with thin liquids than with thicker textures. Some children prefer sour or spicy food over bland food, crunchy vs. smooth, cold vs. warm, or vice versa. These attributes usually interact and have effects on the efficiency and pleasure of feeding.
Does the feeding problem change throughout the course of the meal?
It is not unusual that children who are orally defensive demonstrate little to no hunger, have poor appetites, have postural problems, and have breakdowns in child-parent interactions. They often show more difficulty before or at the beginning of meals and may improve as the meal progresses. Children with oral sensorimotor and swallowing deficits may demonstrate more problems near the end of the mealtime due to fatigue, compromised cardiopulmonary function, and oropharyngeal dysphagia.
Does the feeding problem vary by time of day or by feeder?
Environmental factors that can alter mealtime efficiency need to be explored. These environmental factors may involve different approaches or methods by different caregivers, possible distractions at mealtimes (e.g., other children, television, pets), appetite suppressants, and fatigue factors.
Does the child maintain a midline neutral position of the trunk, neck, and head without requiring added support?
If the answer is no, what are the interfering factors? Some children with cerebral palsy as well as those with other neurologic diagnoses may show extensor arching of the trunk and extremities while feeding. The risks for aspiration may be greater with this posture than for the child who sits upright with good head control. At the other extreme is the child with hypotonia who has a "floppy" neck. That child may have increased risk for aspiration because of excessive flexion of the oropharynx due to the "floppy" neck.
Are there signs of breathing difficulties during feeding?
These signs may include rapid respiratory rate, panting (especially in infants while sucking and swallowing via nipple), increased nasal congestion, and gurgly voice quality. Any changes in respiratory effort and/or rate should be investigated. The work of breathing takes precedence over the work of feeding. Signs of possible risks for aspiration with oral feeding must be followed up with appropriate investigations, e.g., videofluoroscopic swallow study (VFSS), flexible endoscopic examination of swallowing (FEES), esophagogastroduodenostomy (EGD), esophageal manometry, and computed tomography (CT) scan of the chest.
Does the child have emesis regularly?
If yes, when does it occur? Can parents estimate the volume per episode? Can parents predict the timing of emesis in relation to feeding? Does the child "spit up" or have projectile vomiting? Children with neurologic-based dysphagia have a high incidence of gastroesophageal reflux (GER) that ranges from 15% to 65%. On the other hand, it is not unusual for children with gastroesophageal reflux disease (GERD) to have no emesis.26
Does the child refuse food?
If yes, when, where, and how often? What are the behaviors of refusal? Food refusal can occur for multiple reasons, some of which are physiologically based and others that may be skill or behavior based. Physical/physiologic problems may have resolved some time in the past, but the negative experiences have been so powerful that the child associates pain and discomfort with eating long after resolution. Factors may relate to one or more of the following: airway, gastrointestinal (GI) tract, oral sensorimotor, and behavior (e.g., parent–child interaction problems). Infants and young children have limited ways to communicate their stresses. Thus, food refusal may be the way the child can let others know about pain or discomfort, or possibly the child may be exerting independence and control.
Does the child get irritable or sleepy and lethargic during mealtimes?
Irritability is one way that problems with GER, other gastrointestinal problems, and airway problems are communicated. Irritability can also be a behavior response, but that is less likely than a physiologic response. Lethargy at mealtime may relate to excessive fatigue, recurrent seizures, or medications with sedative effects (e.g., anticonvulsants, muscle relaxants).
How do the child and caregiver interact? Are there signs of forced feeding?
Parental stress related to the feeding situation can be transmitted to a child, which in turn exacerbates the feeding difficulties. Forced feeding seldom leads to feeding success. Complications are more apt to follow [e.g., food refusal, failure to thrive (undernutrition), and other more global behavior maladaptations].
Top of page
Interdisciplinary Team Approach
An interdisciplinary team approach offers the benefit of coordinated consultation and problem solving for multiple interrelated problems. Effective management of these medically complex children depends on the expertise of many specialists, who may work independently and as a team (Table 5). Case coordination is often a critical component that is intensive and needed to optimize the child's health and development along with the family's ability to cope with multiple issues and sometimes disparate opinions and recommendations. An interdisciplinary approach is recommended at institutions where professionals evaluate and treat children with complex feeding and swallowing problems. Success factors include the following:
- Collegial interaction among relevant specialists
- Shared group philosophy related to diagnostic approaches and management protocols
- Team leadership with organization for evaluation and sharing of information
- Willingness to engage in creative problem solving and research
- Time commitment for the labor-intensive work that is required
Depending on the expertise and interest in different institutions, team members may be drawn from different disciplines. The functions should cover those described (Table 5). Not all disciplines will be needed for all children. It is important to determine which disciplines can best serve the child and family so that patient care can be both efficient and efficacious. Specific discipline involvement may change over time as the child's needs change.
Top of page
Instrumental Examination of Swallowing
Instrumental examinations may be needed for infants and children particularly when the pharyngeal and esophageal physiology needs to be delineated objectively to answer specific questions related to the safety and efficiency for oral feeding. Criteria for instrumental examinations of swallowing include, but are not limited to:
- Risk for aspiration by history and clinical observation
- Observation of infants demonstrating incoordination of sucking, swallowing, and breathing during oral feedings at breast or bottle
- Clinical observation of older children with a variety of signs suggesting possible pharyngeal or upper esophageal phase swallowing deficits
- Prior aspiration pneumonia or similar pulmonary problems that could be related to aspiration
- Suspicion of pharyngeal or laryngeal problem on basis of etiology, particularly neurologic involvement that is common with feeding and swallowing problems
- Gurgly voice quality
- Need to define oral, pharyngeal, and upper esophageal phases of swallowing
Multiple factors are considered in making decisions about which examination and when it will be used. The decision regarding which instrumental examination is needed depends on the anatomic areas and functional processes to be assessed. Instrumental methods for evaluation of swallowing include videofluoroscopic swallow study (VFSS), flexible endoscopic examination of swallowing (FEES), and ultrasonography (US). Specific diagnostic questions can be answered to guide therapeutic decisions. Other diagnostic assessments that do not measure swallowing directly may influence recommendations related to swallowing (e.g., scintigraphy or salivagram).
Considerations for Instrumental Examinations
Protocols for and interpretation of VFSS need to be developmentally appropriate for the infant or child at baseline health status and not during an acute illness or when unstable medically. Other considerations include developmental function levels, positioning, bolus presentation, viscosity of bolus, respiratory rate, and swallowing variability.27 Fiberoptic nasopharyngolaryngoscopy (FNL) with infants is primarily for assessment of the anatomy and physiology of the upper aerodigestive tract. Observations of swallows may be incorporated as needed. A modification of this procedure, FEES, is focused directly on observing the pharyngeal phase of swallowing, although it is less complete than VFSS; FEES can include sensory testing.28 Ultrasonography has been used to study sucking and oral transit in breast-fed and bottle-fed infants. Although US provides capabilities for observations of the feeding process in an environment that does not require radiation or insertion of a scope, it has not been used extensively to date for clinical purposes in the United States or in other parts of the world, but more for research. In general, infants and children are referred for instrumental assessment when they are physiologically stable and when the clinical findings or history indicate possible swallowing or related abnormalities that will impact decision making regarding oral feeding.
Interpretation of Findings
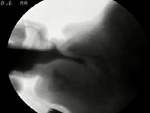
Interpretation of instrumental findings is made in conjunction with the history, clinical findings, and other health-related issues. It is of interest to note that typically developing children who experience a traumatic choking event or have pain with swallowing during an acute illness may stop eating all solid food, lose weight, and become fearful of the entire eating experience. Some gain confidence to resume normal oral eating once they have viewed the video of their swallowing during a VFSS and can see that there is nothing blocking the movement of the food going through their pharynx and into the esophagus. If they do not resume typical eating and drinking, additional issues are likely to need resolution through intervention related to psychological issues or further workup for other possible underlying physical or physiologic problems. Examples of VFSS cases may be seen in Videos 1, 2 and 3.
Video 1: Normal swallowing in infants (Normal Study)

This infant, nearly 5-months old, was referred for VFSS because of concerns related to "spitting up frequently and sounding gurgly after feeds". He was on medication for gastroesophageal reflux. Infant was positioned semi-upright in his typical feeding posture in a seat for a lateral view of oral, pharyngeal, and upper esophageal phases of swallowing. The sequence of swallows in this segment were made as he sucked on the milk bottle nipple that has been used at home.
Note that initially this infant sucked two times before he swallowed. Within the first few swallows, he settled into a 1:1 suck:swallow ratio, which is the most efficient for infants. This infant had no aspiration or nasopharyngeal penetration. As the study progressed, he had occasional laryngeal penetrations only to the underside of the epiglottis. He cleared the pharynx with completion of each swallow. If this infant maintains the pattern demonstrated in this examination throughout feedings, there is no obvious reason that any respiratory concerns would be directly related to his swallowing mechanism.
- View movie file : Video 1: Normal swallowing in infants (Normal Study)
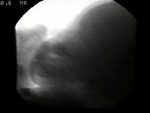
Video 2: Grossly abnormal swallowing in an infant. (Severe pharyngeal phase dysphagia.)
A 7-month-old infant was referred for VFSS by her primary pediatrician because of concerns related to risks for aspiration while feeding orally. She was a term infant with intrauterine growth retardation. An upper GI examination a few days prior to this examination had revealed occasional silent aspiration with swallowing, gastroesophageal reflux, and mild gastritis, and vomiting. She had mild developmental delays with hypertonicity.
This infant was very eager to take her bottle. This section of the VFSS shows multiple aspiration events with the first aspiration occurring at the initiation of the fourth swallow. The aspiration appeared most closely correlated with timing and coordination deficits. With increased residue in the pharynx, particularly in the pyriform sinuses, she also aspirated as residue spilled into the open airway following some swallows. She made no response to the aspiration, but she kept sucking eagerly. She fussed when the nipple was taken out of her mouth. Thickening liquid did not eliminate aspiration events. She did not aspirate with spoon feeding (not shown in this section).
- View movie file : Video 2: Grossly abnormal swallowing in an infant. (Severe pharyngeal phase dysphagia.)
Video 3: Abnormal swallowing resulting in delayed aspiration. (Occasional aspiration)
This 6-month-old infant was referred for VFSS because of concerns related to vomiting during and apart from feedings as well as choking and coughing during nipple feeds. History was significant for intrauterine drug exposure that included cocaine and methamphetamine throughout the pregnancy. He has been in foster care since the newborn period. Thickened feeds had not helped reduce vomiting. An UGI examination 2 weeks prior to this examination revealed nonobstructive upper GI with gastroesophageal reflux.
He was positioned for bottle feeding and lateral view with foster mother presenting his formula with milk bottle nipple used at home. His suck-to-swallow ratio varies from 1:1 to 3:1, which is basically efficient for taking sufficient volume to meet caloric needs. Note that when he sucks multiple times before swallowing, the liquid is seen deeper in his pharynx (to the pyriform sinuses) resulting in a brief delay in initiation of a pharyngeal swallow. When that pattern is seen, one gets suspicious for potential aspiration as an infant continues to suck and swallow. Therefore it is important to observe more than just a few swallows with bottle feeding. By the 16th swallow, aspiration occurred as he was initiating a swallow. There was no cough. He continued to suck and swallow, with additional aspiration events. Near the end of this section, the nipple was removed and you can tell that he produced a delayed cough, but he did not clear his airway.
- View movie file : Video 3: Abnormal swallowing resulting in delayed aspiration. (Occasional aspiration)
Flexible Endoscopic Examination of Swallowing (FEES)
For infants and children, a pediatric otolaryngologist and speech-language pathologist typically perform the FEES together as a team. Swallowing function parameters evaluated include pharyngeal pooling of secretions, premature spillage into pharynx, laryngeal penetration, aspiration, residue, vocal fold mobility, gag reflex, and laryngeal adductor reflex (LAR). Major disadvantages include incomplete examination of the pharyngeal phase of swallow, lack of visualization of the oral or esophageal phases of swallowing, and thus the inability to evaluate coordination of pharyngeal motility with tongue action, laryngeal elevation or excursion, and upper esophageal opening. When airway concerns are prominent, FEES is preferable to VFSS to assess airway safety even prior to oral intake. FEES can be performed at the bedside, which can be a major advantage for some infants and children. This examination requires the child's cooperation, just as the VFSS does in order to have reliable and valid findings that should help to clarify the oral feeding status. This examination may be particularly useful for children with developmental disabilities and neurologic impairments.
Top of page
Management of Feeding and Swallowing Problems in Pediatrics
Management decisions are made in light of the total child with consideration for medical/surgical, nutrition, oral sensorimotor, behavioral, and psychosocial factors. Intervention strategies are focused on primary problem areas of deficit. Evidence-based practice guidelines are needed. Airway stability and adequate nutrition/hydration status are prerequisites for all oral sensorimotor and behavioral approaches to increase the volume of oral feeding or to improve oral skills to expand food textures and to increase efficiency. Initial efforts to improve caloric intake may include increasing caloric density of food, as per the dietitian and physician, along with making adjustments of food textures to improve efficiency and safety of oral feeding. Adequate fluid intake is critical to meet hydration needs and to minimize potential of constipation, which can be a major complicating factor in facilitating hunger, appetite, and interest in feeding.
Oral sensorimotor intervention involves strategies related to the function of oral structures for bolus formation and oral transit that are under voluntary neurologic control, that is, the jaw, lips, cheeks, tongue, and palate. Techniques vary widely among therapists with little evidence of efficacy, efficiency, and outcomes. Some children appear to improve oral function when foods vary on the basis of texture, tastes, and temperature. Other children show significantly improved oral skills and timing of swallowing with posture and position changes. Frequently used strategies include tapping or stroking the face and using a "Nuk ®" brush or other kinds of stimulation. Parents and therapists report that this kind of stimulation will "wake up the system" and then the child will swallow more quickly and more firmly. However, data are sorely lacking. Goals of specific exercises usually relate to improved strength and coordination, but without defined objective measures of outcomes.
Professionals and parents do not disagree about the importance of adequate nutrition/hydration. However, there is more likely to be disagreement regarding the need for a gastrostomy tube (GT). It is not unusual for parents to need some time, at least a few weeks or even months, before they agree to a GT. A nasogastric (NG) tube may be used for a few weeks as a test to determine if the child tolerates needed volume of liquid per feeding time without discomfort or emesis. The NG tube feeds also provide an opportunity to monitor weight gain. If nonoral feeds are likely to be required for longer than several weeks, not necessarily for total oral feeding but perhaps just to meet fluid requirements or for medications, a GT should be considered. A feeding gastrostomy tube often relieves stress on the caregivers by allowing freedom from fear of malnutrition. More efficient caloric delivery also frees time for other more pleasurable interactions with the child. Some oral therapy should continue at appropriate levels to ensure the continued experience and maximal development of oral skills over time. Speech-language pathologists can train parents, who can then take advantage of offering tastes during several brief "practice" sessions each day. Duration of each session should be only about 5 to 10 minutes in these circumstances. When a child is on bolus feeds, optimal timing for "pleasurable practice" is likely to be shortly before the start of the tube feeding, providing the child does not show aversive reactions to the tube feedings.
Data on evidence-based research are needed. All therapeutic approaches have a primary goal for each child to experience healthy, safe, and pleasurable oral feeding, whether the child is a total oral feeder or gets just limited quantities and types of food for practice and pleasure. Pulmonary stability and nutritional well-being are always the primary goals for all infants and children.
Article related content
Do Babies Aspirate at Some Feeds and Not Others
Source: https://www.nature.com/gimo/contents/pt1/full/gimo17.html
0 Response to "Do Babies Aspirate at Some Feeds and Not Others"
Post a Comment